Dupuytren's disease (Dupuytren's contracture or Dupuytren disease)
Dupuytren's contracture, also abbreviated as Dupuytrens, is a benign thickening of the palm's deep connective tissue (fascia). Often the tumor is located in the flexible area of the skin in the vicinity of the base joints of the fingers. Tumors that start in the lower palm, further towards the wrist, an area known as the palmar aponeurosis, are typically less critical and do not lead to contraction. Although this disease is named Dupuytren's contracture the term Dupuytren's disease (or Dupuytren Disease) might be a better term because it includes the initial stage before the contracture has started.
Can it be cured?
More than 180 years have passed since 1831 when Baron Guillaume Dupuytren (1777-1835) presented his findings in Paris on the disease that acquired his name. Yet the root causes of Dupuytren's disease still remain unknown and the disease cannot be cured. Current treatments are either aiming at slowing down disease progression or improving hand function. Dupuytren's disease is a benign disease, not a lethal one, that affects the - important - finger function.
How does it develop?
Dupuytren's contracture, or rather Dupuytren's disease, typically starts on the palm of the hand with a small nodule or several nodules that can be felt (palpated) and are initially not very hard. There is indication that the disease actually starts earlier with changes in the tissue underlying the skin. Because those changes are on a microscopic level, they generally are not noticed and nodules are usually the first indication of Dupuytren disease.
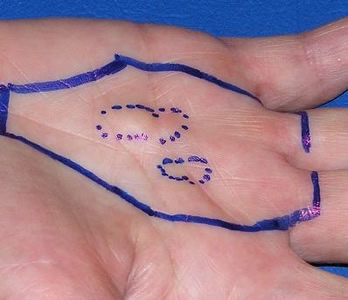
Early symptoms of Dupuytren's
Small nodules in the palm of the hand (dotted lines). No contracture of fingers (the full line indicates the field for radiotherapy; University of Erlangen, Germany).
|
The skin in the palm starts pulling in. Originally there had been a nodule that now begins the "convolution phase" (picture by IDS).
|
Dupuytren's develops at the base of the little finger (circle) and a cord grows into the palm (arrow). Picture by IDS. |
Small Ledderhose nodule on the solel of the foot. Picture by M. Herkstroeter, Frankfurt, Germany. Further examples see below. |



The next stage is the development of cords along tendons. In most cases the fourth or fifth finger is affected first but nodules can also appear throughout the palm, sometimes in the digits, and in rare cases even elsewhere. Typically Dupuytren's disease tends to stabilize temporarily, but the nodules and cords start growing again by degrees over several years. Eventually, as the cords thicken, the contractive forces increase and bend the affected fingers towards the palm (there is actually some indication that there is no real contraction but that the relaxed, bent finger position is fixed by the cord and thus creates an extension deficit. The effect is the same: the finger can't be stretched anymore, resulting in Dupuytren's contracture). A more detailed description of the growth process and the related pathophysiology of Dupuytren's contracture can be found in e-medicine-Revis. Note that the still frequent diagnosis "contracted flexor tendons" for Dupuytren's contracture is somewhat misleading because it is not the tendons that contract.

Example of Dupuytren's and Ledderhose nodules at hand and foot, respectively.
Early stage (stage N of Dupuytrens), no finger contraction
and Ledderhose nodules still relatively small.
(Picture provided by Alfried Krupp Hospital, Essen, Germany)
Below is an example of Dupuytren's contracture in a progressed stage. The finger has been bent permanently into the palm. The skin at the contracted joint thus is less exposed to air and is difficult to keep sufficiently dry and clean. In this case this had already caused skin damage. After treatment (in this case with NA) the finger became straight again and the skin recovered.

Dupuytren's contracture in progressed stage with already damaged skin.
(Picture provided by A. Meinel, Dupuytren Ambulanz, Germany)
Eventually, in rare cases the Dupuytren cord can become very rigid and ossificated Dupuytren cord calcification.
Important to know
Dupuytren Disease can develop into contracted fingers but that is rather an exception than the rule! Most patients with symptoms of early Dupuytren's will never need any treatment in their life. Yet there is a minority of patients suffering from a more aggressive form of Dupuytren's Disease who develop the above later stages and contracted fingers. For those the treatments described on this web site (see Stages and Therapies) can provide relief from troublesome symptoms. Unfortunately, it is still difficult, if not impossible, to predict who is suffering from aggressive Dupuytren Disease and who is not.
It is equally important to be aware that even with a developed Dupuytren's contracture the hand function maybe affected but Dupuytren's is still not a lethal disease. It may affect daily life to some extent but it is important to not let it affect the joy of living.
Nan, a patient in our forum, recently posted below execellent advice link
"Until you have spent some time with this disease it is difficult to know what category of DD individual you will become. Majority of people with this disease have very little problem with it. I have seen hands with enormous nodules and protruding cords where the individual has zero difficulty doing anything. My own husband did not even know he had DD until I was diagnosed, and nodules, he assumed were calluses, were discovered. DD has had no effect on his ability to do whatever he wants with his hands.
Then there is the minority group, those who truly struggle in navigating this disease from when it begins and onward. Most likely this Forum began as a result of those people. If, however, everyone who had DD experienced pain, eventual contraction, limited hand strength, and other various symptoms this Forum would have hundreds of posts a day. It doesn’t take much hand stress for some in the minority group, like myself, to trigger another nodule, or irritate an existing one or cord.
And, of course, there are a host of those who lay somewhere between the two groups.
Others have shared that this disease flares and then subsides for periods of times, or it can slowly progress hardly noticeable.
Also, keep in mind there is Dupuytren and Dupuytren's Contracture.
The question you have to eventually answer and discover is, "Which kind of DD person am I?" That will come from time and observation of how your hands react to various activities, not someone else’s. It seems it would always be sensible whenever diagnosed with a new disease to proceed with caution, until you know what course this disease takes in YOUR life.
Here’s hoping you are in the majority group!
Nan"
Is Dupuytren disease painful?
In most cases Dupuytren's is inconvenient but not painful. Yet, if the nodule or cord affects nerves, then this may indeed become painful. A medical paper reports "Although Dupuytren disease is generally considered painless, we treated a series of early stage patients with painful disease. Intraoperative inspection and histological examination of tissue samples showed that nerve tissue was involved in all cases." (A.von Campe et al. "Painful nodules and cords in Dupuytren disease" J Hand Surg Am 37 (2012):1313-8; abstract).
Ledderhose disease is generally more painful because the nodules in the foot, when grown big enough, get pressured when walking.
What might be causing Dupuytren's disease?
There is evidence that an inclination (predisposition) for Dupuytren's contracture can be inherited (S. Hindocha et al. "The heritability of Dupuytren's disease" J Hand Surg [Am]. 2006 Feb;31(2):204-10 abstract). Some additional environmental effect might be required to start the disease (HA Lyall "Dupuytren's disease in identical twins" J Hand Surg [Br]. 1993 Jun;18(3):368-70 abstract). Damage (or rather healing) of the hand can trigger Dupuytren's disease (see also Dupuytren's work related?). There is some indication that Dupuytren's contracture is a chronic inflammatory disease (full_text).
Oxidative stress in combination with microvessel ischemia (local restriction in blood supply) might be a mechanism driving the onset of Dupuytren's disease, see GA Murrel, FJ Francis, and L Bromley "Free radicals and Dupuytren's contracture" Br Med J (Clin Res Ed) 295 (1987) p 1373 - 5 abstract and IS Yi, G Johnson, and MS Moneim "Etiology of Dupuytren's disease" Hand Clin 15 (1999) p 43 - 51 abstract .
Tension in the palm (palmar fascia) has also been proposed as a factor causing Dupuytren's disease. In a small trial 27 patients had surgical fasciotomy with 13 having a Z-plasty cut reducing post-Op tension. After 2 years 2 patients of that group (15 %) exhibited recurrence while 7/14 (50 %) of the other group, where only a simple transversal cut was used, exhibited recurrence. This might confirm the effect of tension. N. Citron and A. Hearnden "Skin tension in the aetiology of dupuytren's disease; a prospective trial" The Journal of Hand Surgery: Journal of the British Society for Surgery of the Hand 28 (2003) p 528-530 abstract.
Efforts to identify the gene(s) causing Dupuytren's disease have yielded contradictory results Miami_abstracts. A more recent genome wide association study (GWAS), published in 2011, indentified several genes associated with Dupuytren's Wnt_signalling_full_text (and won the Dupuytren Award 2012). Further studies are under way, but this is far from offering a cure. However, even without knowing all genes involved, we already know much more about the symptoms of the disease and we have made some progress in treating it.
Are alcohol consumption and smoking risk factors?
The results of various studies on the effect of alcohol consumption on Dupuytren's disease are in conflict. Heavy drinking seems to make the disease worse while statistical research of a large numbers of Dupuytren's patients did not exhibit a higher percentage or level of alcohol consumption than in the normal population. Yet recently prevalence studies in the Netherlands exhibited a clear and measurable effect on the probability to develop Dupuytren disease (or the prevalence) when drinking just 2 units of alochol per day (either glasses of beer or wine) R. Lanting et al. "Prevalence of Dupuytren Disease in The Netherlands" Plast Reconstr Surg. 2013 Aug;132(2):394-403 abstract. Drinking more increases the probabilty further. - Smoking may cause an earlier onset of the disease as revealed by a patient survey http://www.dupuytren-online.info/patient_survey.html. For smokers both diseases, Dupuytren's and Ledderhose, started 7 years earlier on average.
Risks of developing Dupuytren Disease when taking certain medications are decribed on page "Stages and therapies"
Are there diseases related with Dupuytren Disease?
Ledderhose's disease is similar to Dupyutren's contracture except that it affects the feet, typically starting with nodules in the arch (plantar aponeurosis).
A possibly related disease affects the male genital (Peyronie's disease, induratio penis plastica, IPP). For further information see http://www.dupuytren-online.info/IPP_and_others.html and the further pages in that section.
History of Dupuytren's research and treatment
A good overview of the history of Dupuytren disease is provided on the website of the British Dupuytren's Society http://dupuytrens-society.org.uk/stories/history/ and http://dupuytrens-society.org.uk/hand-problems-and-miracle-cures/ .
Continued:
Age distribution and prevalence in various countries
Stages and therapies of Dupuytren's disease
Dupuytren's contracture and trauma
Literature on Dupuytren's disease
Page last modified:
12/30/2020